Dr. Boerger, Thomas
Facharzt für Orthopädische Chirurgie und Traumatologie



Our hands are essential tools in our daily lives. We use them constantly for work, everyday tasks, and even communication.
When an injury or illness affects mobility or causes pain, our quality of life is seriously affected.
Fortunately, hand surgery can solve many of these problems, restoring functionality and eliminating discomfort. Below, we explain the most common interventions and when they may be necessary.

An early diagnosis can make a significant difference in your recovery. regain the full functionality of your hands.

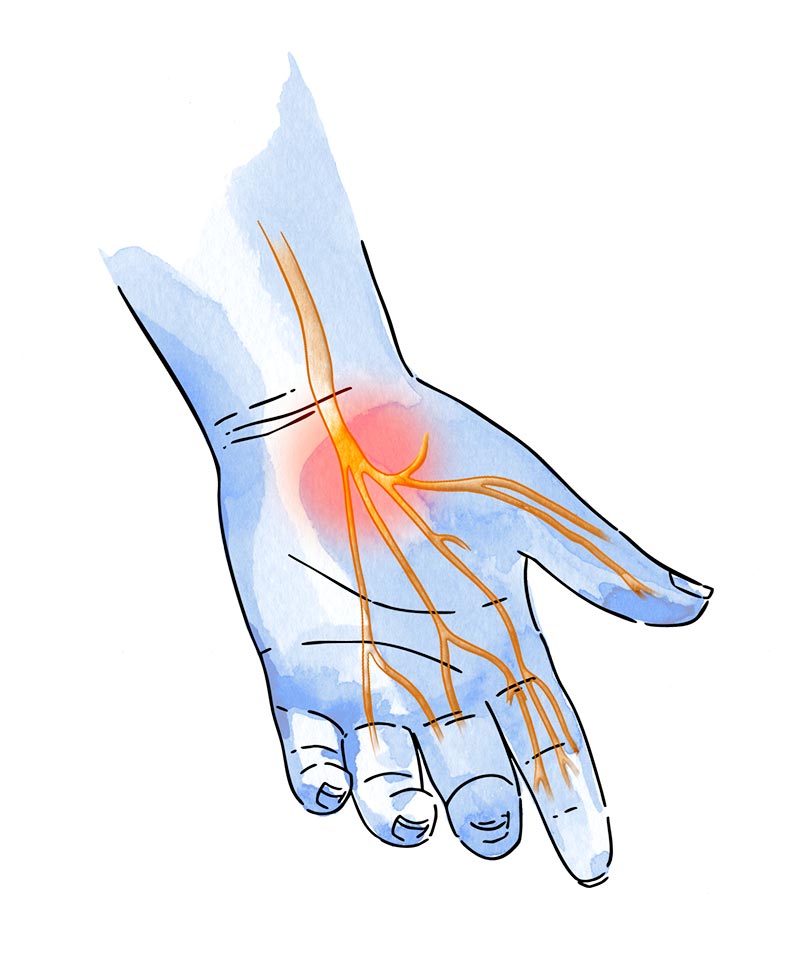
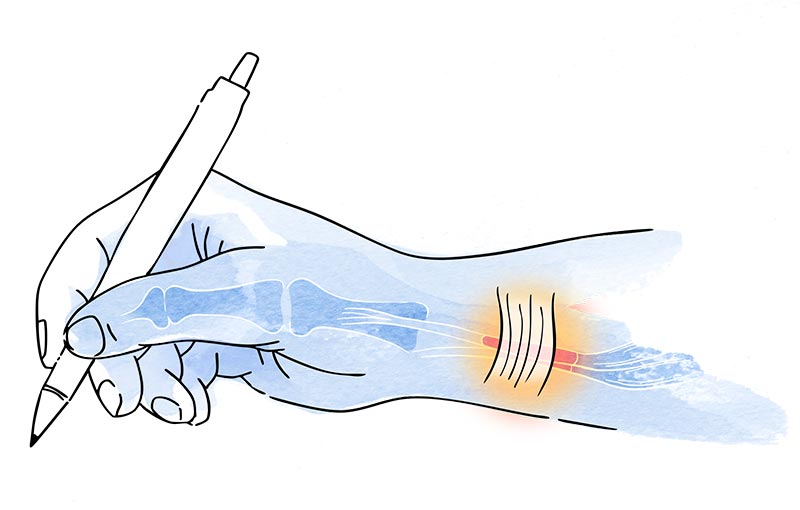
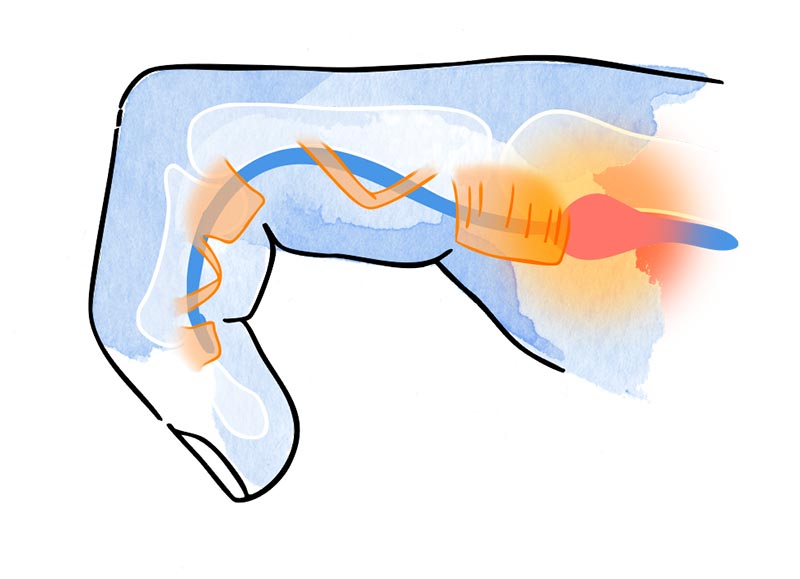
Carpal tunnel syndrome is one of the most common hand conditions. It occurs when the median nerve, which runs through the wrist, becomes compressed due to inflammation of the surrounding tissues.
- Tingling in the thumb, index, and middle fingers.
- Nighttime pain that requires moving the hand to relieve it.
- Weakness in the hand.
- Difficulty holding small objects.
In the early stages, treatment is often non-surgical. Wearing a night splint to keep the wrist in a neutral position can help reduce pressure on the median nerve. Anti-inflammatory medications or corticosteroid injections may also be used to reduce inflammation. In some cases, physiotherapy and modifying the activities that trigger symptoms can help relieve pain and improve function.
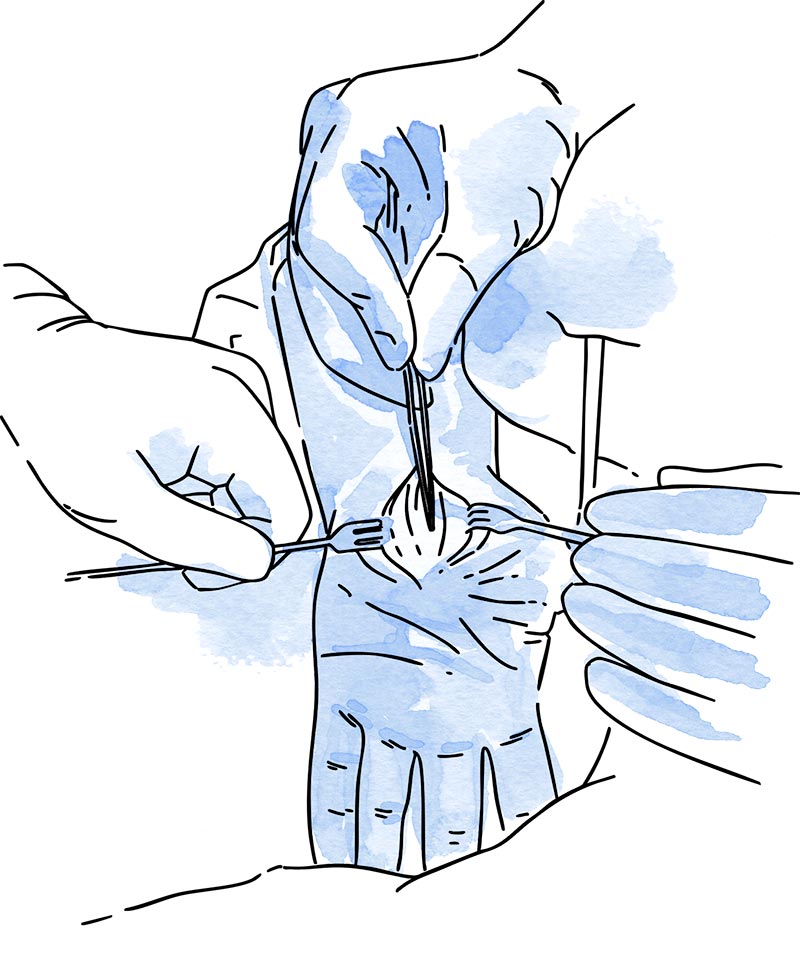
If symptoms persist and do not improve with conservative treatment, surgery is recommended.
The procedure involves releasing the median nerve by cutting the ligament compressing it. It is performed under local anesthesia and is a quick procedure with easy recovery.
This disease affects the palmar fascia, a tissue located right beneath the skin of the palm. Over time, nodules and fibrous cords form, pulling the fingers toward the palm and preventing them from extending properly.
- A lump or nodule appears in the palm of the hand.
- The fingers (especially the ring and pinky fingers) begin to bend, making them impossible to fully extend.
- It doesn’t usually cause pain, but significantly limits hand function.
In early stages, when retraction is still mild, a conservative approach may be considered. Although it does not stop the progression of the disease, using night splints or performing specific exercises under the supervision of a physiotherapist may help preserve mobility. Collagenase injections—an enzyme that weakens the cords—can also be used to rupture them in a less invasive manner.
In selected patients, a needle fasciotomy may be an option. This minimally invasive technique involves severing the fibrous cords through small punctures in the skin or even without making an incision. The procedure is performed under local anesthesia, allows for a quick recovery, and is ideal for localized contractures with minimal fibrosis.
When the contracture is advanced or significantly limits hand function, open surgery is the preferred treatment. The standard procedure is an aponeurectomy, which involves removing the affected fibrous tissue to release the fingers and restore extension. This intervention typically requires a longer postoperative recovery but provides lasting results in more complex cases.
De Quervain’s tenosynovitis is an inflammation of the tendons that run through the first dorsal compartment of the wrist, at the base of the thumb. It is common in individuals who perform repetitive hand movements, such as texting, using a computer mouse, lifting babies, or engaging in certain sports.
- Sharp pain at the base of the thumb and along the wrist.
- Difficulty gripping objects or performing pinching movements.
- Worsening of pain with specific wrist and thumb motions
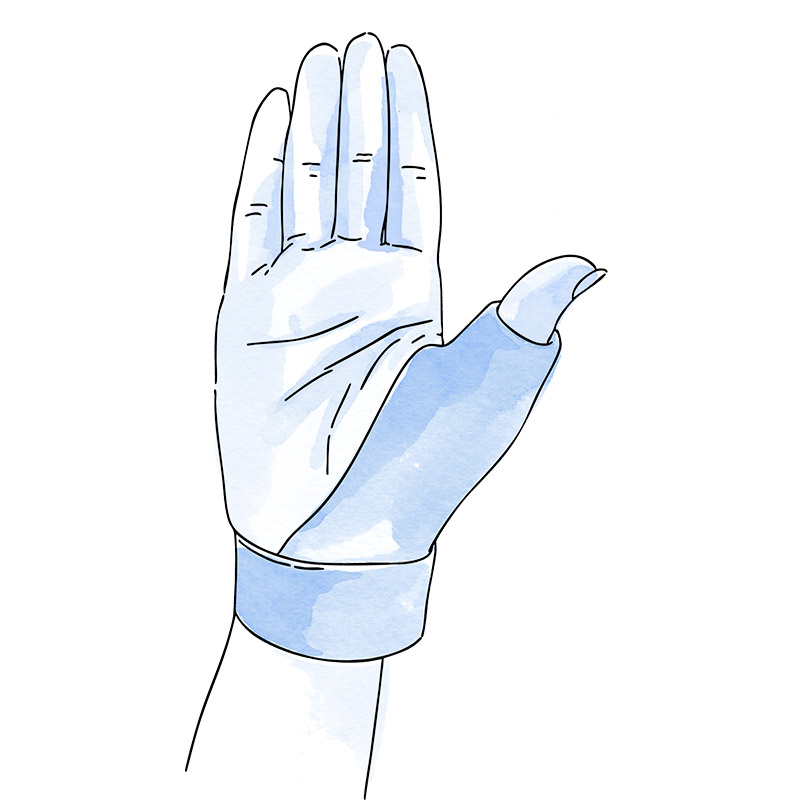
In the early stages, treatment is usually non-surgical. It includes activity modification, use of a splint to immobilize the thumb and wrist, application of cold packs, oral or topical anti-inflammatory medications, and targeted physiotherapy. In persistent cases, a corticosteroid injection into the affected area can provide significant symptom relief.

If pain persists despite conservative treatments, surgery may be indicated. The procedure involves making a small incision along the radial aspect of the wrist to release the tendon sheath that is compressing the tendons. It is performed as an outpatient procedure under local anesthesia, with a quick recovery and effective relief of pain and restoration of thumb function.

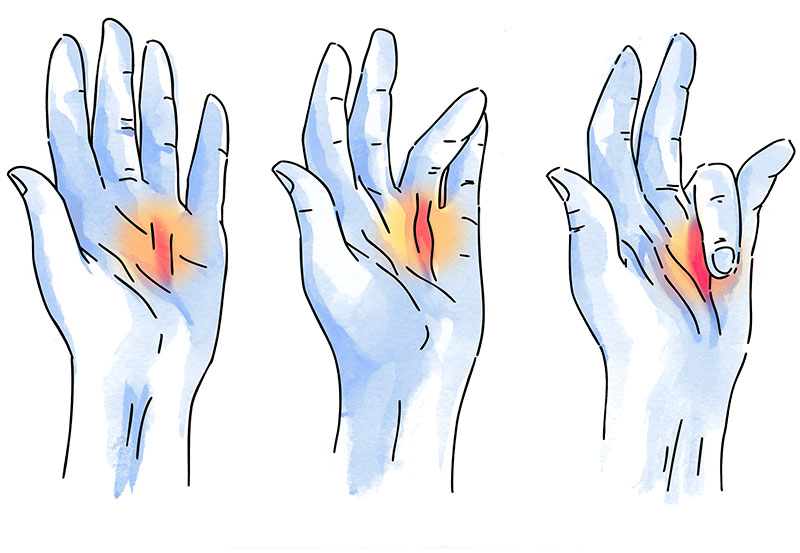
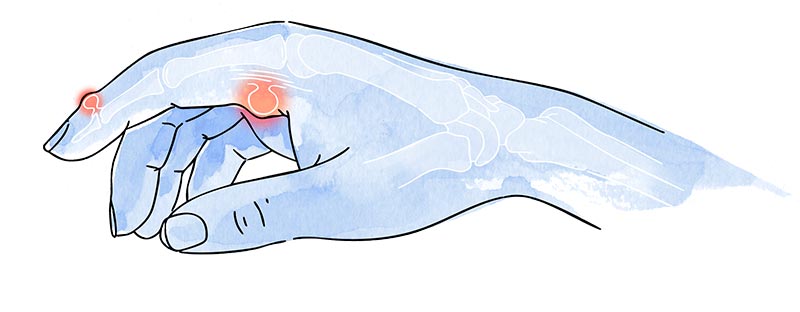
Trigger finger, or stenosing tenosynovitis, occurs when a finger’s flexor tendon becomes trapped in its sheath due to thickening of the tendon or the surrounding fibrous ring (A1 pulley). This leads to a painful catching or locking sensation when trying to straighten the finger.
- A sensation that the finger “catches“ or locks during movement.
- Pain and stiffness, especially in the morning.
- In advanced cases, the finger may remain stuck in a flexed position and require assistance from the other hand to extend.
In mild cases, initial treatment includes activity modification, use of night splints, and anti-inflammatory medications. Physiotherapy and ergonomic adjustments may also help. If symptoms persist, a corticosteroid injection into the tendon sheath can often resolve the condition without the need for surgery.
If symptoms continue or in more severe cases with persistent locking, surgical intervention is recommended. The procedure is performed under local anesthesia and involves releasing the flexor tendon by cutting the A1 pulley. This allows the tendon to glide freely again. Recovery is typically quick, and most patients experience immediate relief from locking and pain.

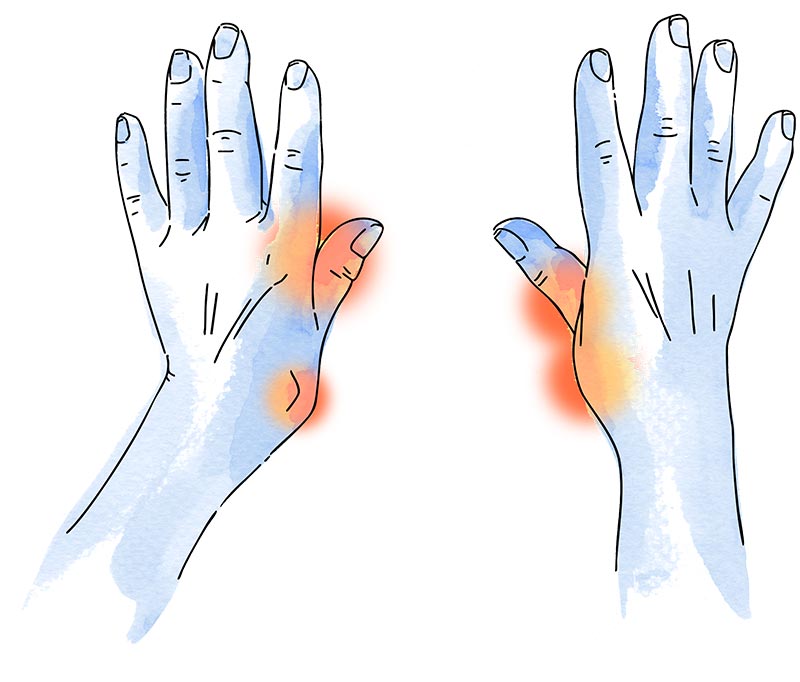
Rhizarthrosis is a type of osteoarthritis that affects the trapeziometacarpal (TMC) joint at the base of the thumb. It results from the progressive wear and tear of the joint cartilage and is a very common cause of pain and functional limitation in the hand, especially among women over the age of 50.
- Pain at the base of the thumb when grasping objects or performing pinching movements.
- Progressive loss of grip strength, particularly when opening jars or turning keys.
- Swelling or visible deformity in advanced stages, often with displacement of the thumb.
In early to moderate stages, conservative treatment can be effective. It includes the use of thumb-stabilizing splints to limit painful movement, physiotherapy to improve function and strengthen the surrounding muscles, and the use of analgesics or anti-inflammatory medications to control pain. Intra-articular injections of corticosteroids or hyaluronic acid may also provide temporary symptom relief for several weeks or months.
Depending on the severity of the osteoarthritis, surgical options may include joint replacement (prosthesis), joint fusion (arthrodesis), or trapeziectomy (removal of the trapezium bone). These procedures aim to reduce pain and restore mobility.
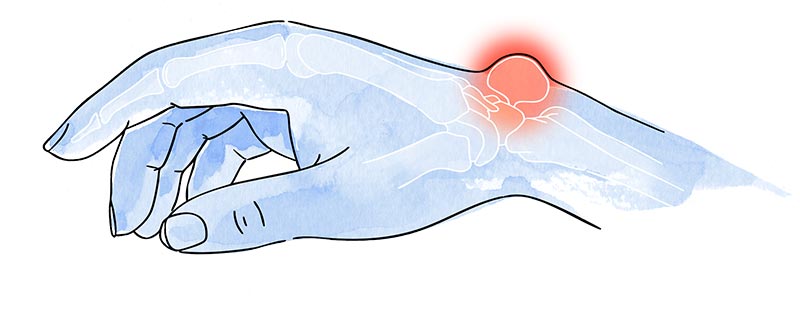
Ganglions, also known as synovial cysts, are benign fluid-filled swellings that develop near joints or tendons, most commonly on the back of the wrist or at the base of the fingers. They are the most frequent type of cyst found in the hand and wrist.
- Appearance of a soft lump on the wrist or at a finger joint.
- Pain or a feeling of pressure, especially if the cyst is large or compresses nearby structures.
- Size fluctuation with activity: tends to enlarge with hand use and shrink with rest.
In many cases, ganglion cysts are asymptomatic and do not require treatment. Active observation is often recommended, as some cysts resolve on their own. For symptomatic cases, aspiration of the cyst’s contents with a fine needle may be performed, although the risk of recurrence is relatively high.
If the cyst causes pain, functional limitation, or recurs frequently after aspiration, surgical removal may be indicated. The procedure involves excising the ganglion along with its pedicle at the joint or tendon origin to reduce the likelihood of recurrence. It is usually performed as an outpatient procedure under local or regional anesthesia.
In addition to treating common conditions, hand surgery also plays a key role in restoring both function and appearance after trauma, previous surgeries, or neurological conditions.
- Sequelae of fractures or poorly healed injuries, resulting in deformities or stiffness.
- Tendon transfers, used to restore movement in cases of paralysis or loss of muscle function due to nerve injury or neuromuscular disorders.
- Soft tissue reconstruction, following accidents, burns, or oncologic surgery.
- Coverage of complex defects using local, regional, or microsurgical flaps.
Each case requires a personalized evaluation by a specialist in hand surgery, as the treatment approach depends on the type of injury, the patient’s prior function, and the desired outcomes. The ultimate goal is to restore movement, relieve pain, and recover hand function and independence.

Dr. Boerger, Thomas
Facharzt für Orthopädische Chirurgie und Traumatologie

Dr. Negru, Marius
Facharzt für Orthopädische Chirurgie und Traumatologie

Dr. Ayllón García, Antonio
Facharzt für Minimal Invasive und endoskopische Wirbelsäulenchirurgie

Dr. Estades Rubio, Francisco Javier
Facharzt für Orthopädische Chirurgie und Traumatologie

Dr. Villanova López, María del Mar
Facharzt für Orthopädische Chirurgie und Traumatologie

Dr. Baczynski, Kamil
Facharzt für Orthopädische Chirurgie und Traumatologie

Dr. Rodríguez García, Miguel Ángel
Facharzt für Minimal Invasive und endoskopische Wirbelsäulenchirurgie
Tel.: +34 952 908 628
+34 609 148 799
952908898 Onkologie
951829978 Bildgebende Diagnostik
951829947 Gynäkologie
952908897 Fertilitäts-Zentrum
951829947 Physiotherapie