

Urinary incontinence is defined as any involuntary loss of urine that causes a social or hygiene problem to the individual. It occurs in healthy people as well as in association with other diseases and can be caused for many reasons.
It is calculated that between 30-40% of middle aged women have some type of incontinence and this percentage increases with age..
The majority of patients, encouraged through the media and advertising, use pads as a method of controlling their incontinence, this has a high cost both economically and ecologically (massive use of cellulose).
It is very important to differentiate between the types of incontinence and to make an accurate diagnosis , as the treatments are very different; we will be discussing the following types:
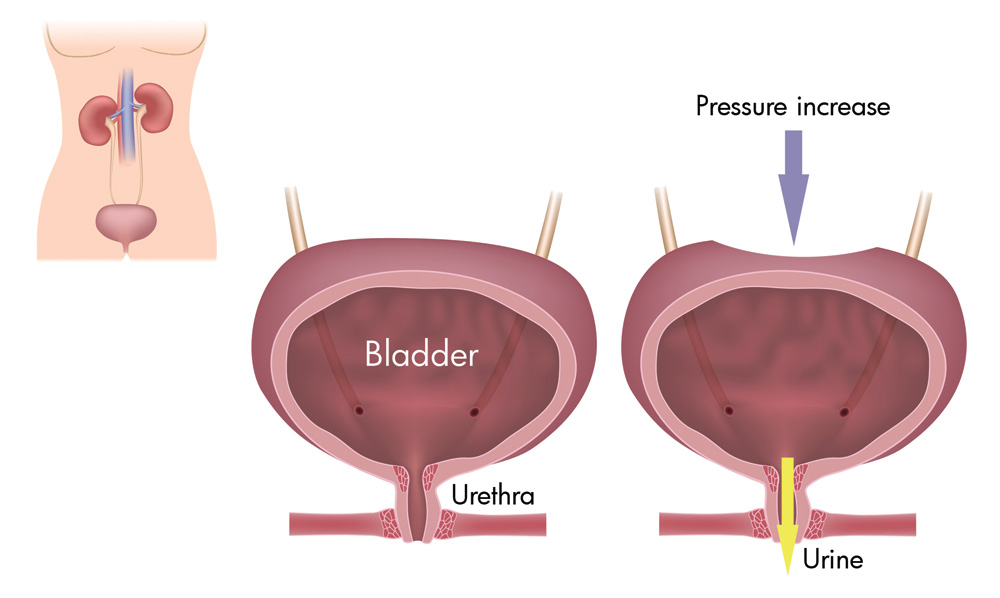
1) Stress incontinence (SI): this is the involuntary loss of urine associated with physical effort that causes an increase in abdominal pressure (such as coughing, laughing, running or walking).
2) Urge incontinence (Overactive Bladder): occurs when the bladder muscle starts to contract and expel urine ahead of time, even if the bladder is still not full.
These contractions can cause a sudden, intense desire to pass urine, causing the involuntary loss of urine. The main symptoms of this are: the need to urinate frequently and the need to pass urine during the night.
This type of incontinence is also very frequent in patients with prostate symptoms.
3) Mixed urinary incontinence.
It is calculated that 30% of women with incontinence suffer from both types previously mentioned.
4) Continuous Incontinence.
Is the involuntary and continuous leakage of urine. This can be due to a vesico-vaginal fistula (a communication between the bladder and the vagina) and usually presents after gynaecological surgery such as a hysterectomy.
5) Other types of incontinence.
There are other types of incontinence but we will not be focusing on them in this article.
Instead we will be focusing on the two most frequent types of urinary incontinence: stress incontinence and urge incontinence. We will be concentrating principally on their treatment which aims to improve the patient’s quality of life.
Treatment should always be individualised, whilst using one or two pads a day does not create a problem for some people, for others even a few drops (for example when exercising at the gym) can be a traumatic event.
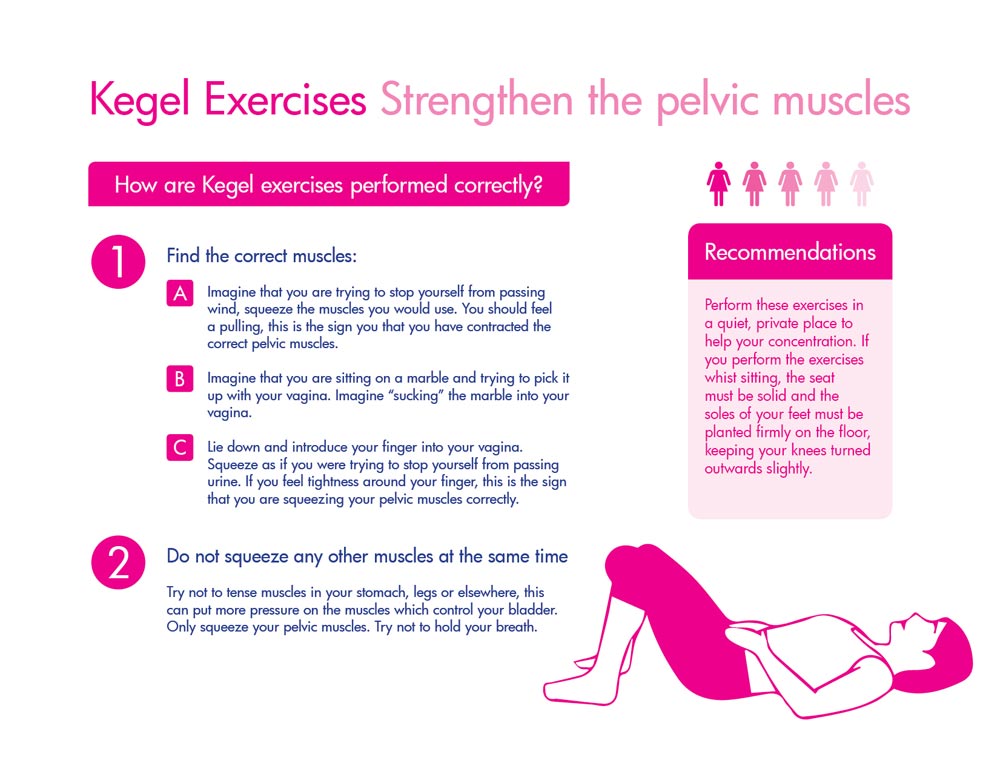
With respect to Urinary Stress Incontinence, the emphasis is on prevention through the strengthening of the pelvic muscles. Kegel exercises (please see the attached table) and the use of Chinese balls (found in pharmacies) are highly recommended for avoiding future stress incontinence.
Kegel exercises and the use of Chinese balls can also reverse incontinence in patients whose incontinence is still mild.
When we talk about incontinence on moderate or minimum effort (coughing, laughing, walking, lifting something heavy) requiring the use of protective measures such as pads. The definitive treatment is surgical, it is a simple operation, through which a sling is positioned under the urethra, this serves as anchorage for all the muscles of the pelvic floor. It is performed under epidural anaesthetic and the patient is in hospital for less than 24 hours, achieving dryness immediately.
In contrast, treatment for incontinence due to a hyperactive bladder is very different to that previously mentioned, there are different levels of treatment for this condition.
New drugs are available which have been demonstrated to be highly effective, with fewer side effects and which can be administered both orally and through skin patches.
There is a group of patients who do not respond to these drugs, for these people we can offer intravesical Neuromodulator injections (these are given on an outpatient basis, with or without sedation, via cystoscopy in about 15 minutes) or percutaneous tibial nerve stimulation.
In summary it is obvious that correctly diagnosing the type of incontinence is critical in formulating the appropriate, individualised treatment plan for the patient, and therefore improving the patient’s quality of life.
TABLE: KEGEL EXERCISES – To strengthen the pelvis muscles
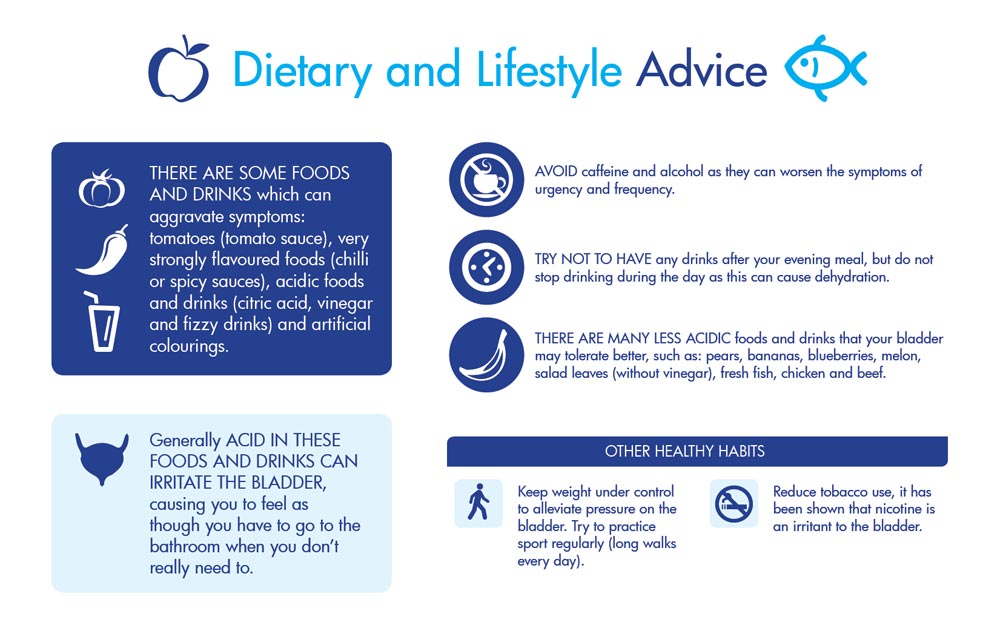
DIETARY AND LIFESTYLE ADVICE
 Dr. José Manuel Fernández Montero
Dr. José Manuel Fernández Montero
Head of Urology Unit
April 6, 2016
Read other news
Tel.: +34 952 908 628
+34 609 148 799
952908898 Oncology
951829978 Diagnosis by imaging
951829947 Gynecology
952908897 Fertility
951829947 Physiotherapy


